Restoring Expression After Brain Tumor Removal
Facial reanimation following acoustic neuroma surgery.
At a Glance
The Challenge
The removal of an acoustic neuroma (a benign brain tumor) can sometimes damage the facial nerve, leading to complete paralysis on one side. This patient lost the ability to smile, close their eye, and express emotion on the affected side, which significantly impacts daily communication and self-image.
The Solution
Dr. Jowett utilized "nerve transfers" to restore power to the facial muscles. This involves rerouting healthy nerves from nearby areas (specifically nerves that normally control chewing (masseter nerve) and tongue movement (hypoglossal nerve)) and connecting them to the facial nerve. This provides a new power source for the facial muscles without causing noticeable deficits in chewing or speaking.
Technical Insight
Procedure: Masseter-to-facial nerve transfer and hypoglossal-to-facial nerve transfer (jump graft or direct).
Surgical Note: This dual-nerve transfer approach reinnervates the facial musculature by recruiting motor axons from the trigeminal (V) and hypoglossal (XII) nerves. The masseter nerve provides a strong motor drive for the midface and smile, while the hypoglossal nerve contributes to resting tone and eye closure. This combination helps restore symmetry and dynamic movement with minimal donor site morbidity.
Donor Options for Nerve Transfer in Facial Reanimation
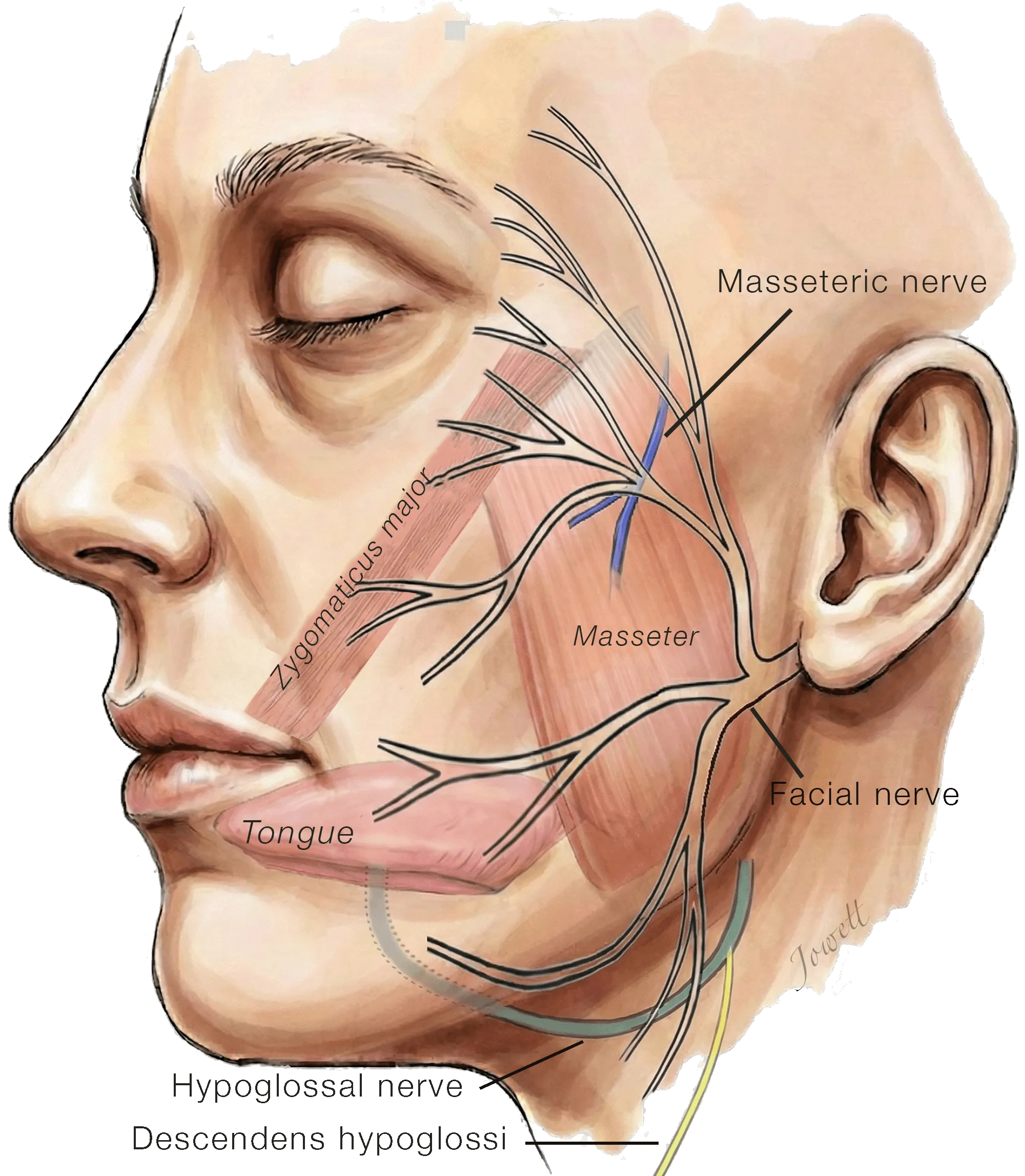
In facial paralysis resulting from injury to the facial nerve near the brainstem, the nerve no longer delivers electrical signals to the muscles of expression. However, the nerve branches within the face itself remain healthy and intact, ready to be reconnected to new power sources to restore tone and movement.
The Hypoglossal Nerve: Located just below the jaw, this nerve controls movement of the tongue. Because of its close proximity and natural redundancy, a portion of this nerve is often used as a 'donor' to restore muscle tone and movement to the face.
The Descendens Hypoglossi Nerve: This nerve controls movement of small muscles in the neck and can serve as an additional power source to restore resting tone to the paralyzed side.
The Masseteric Nerve: Located within the cheek muscle used for chewing, this nerve lies very close to the smile branches. It is often recruited to provide additional power specifically for smiling.
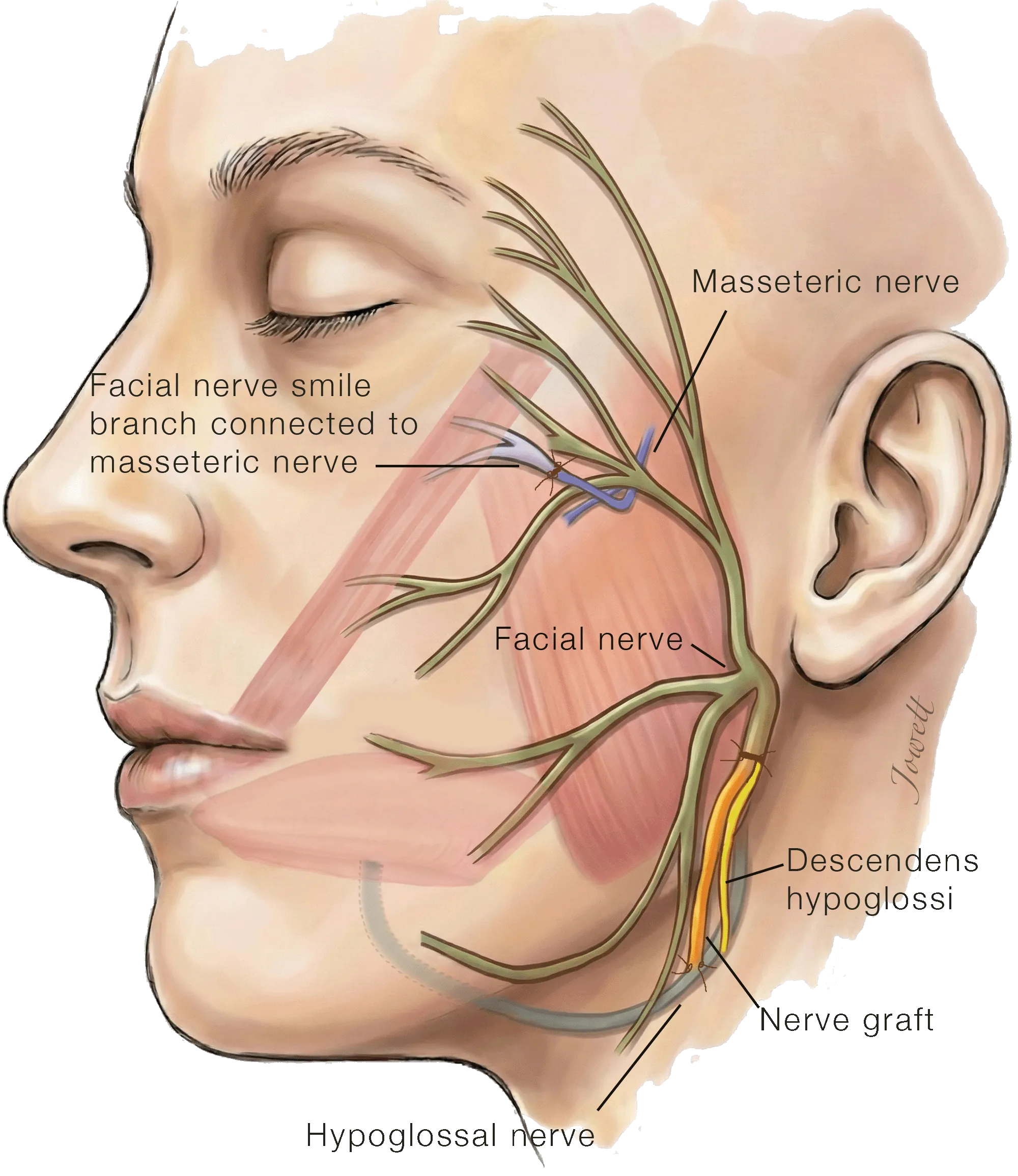
Multiple Nerve Transfer for Facial Reanimation (Hypoglossal, Descendens Hypoglossi, Masseteric)
This diagram illustrates the "rewiring" of the facial nerve. To maximize function, three separate healthy nerves are connected to the paralyzed facial nerve:
For Smile: The masseteric nerve (blue) is connected directly to the facial nerve branch that controls the smile muscles. This provides the strong electrical signal needed to create a smile when the patient clenches their teeth.
For Resting Tone: Both the descendens hypoglossi nerve (yellow) and approximately one-third of the fibers of the hypoglossal nerve are connected to the main trunk of the facial nerve. The descendens hypoglossi nerve is connected directly, whereas a short nerve graft is used to bridge the hypoglossal nerve fibers with the facial nerve. Using both nerves optimizes tone while minimizing the risk of speech or swallowing issues after surgery.
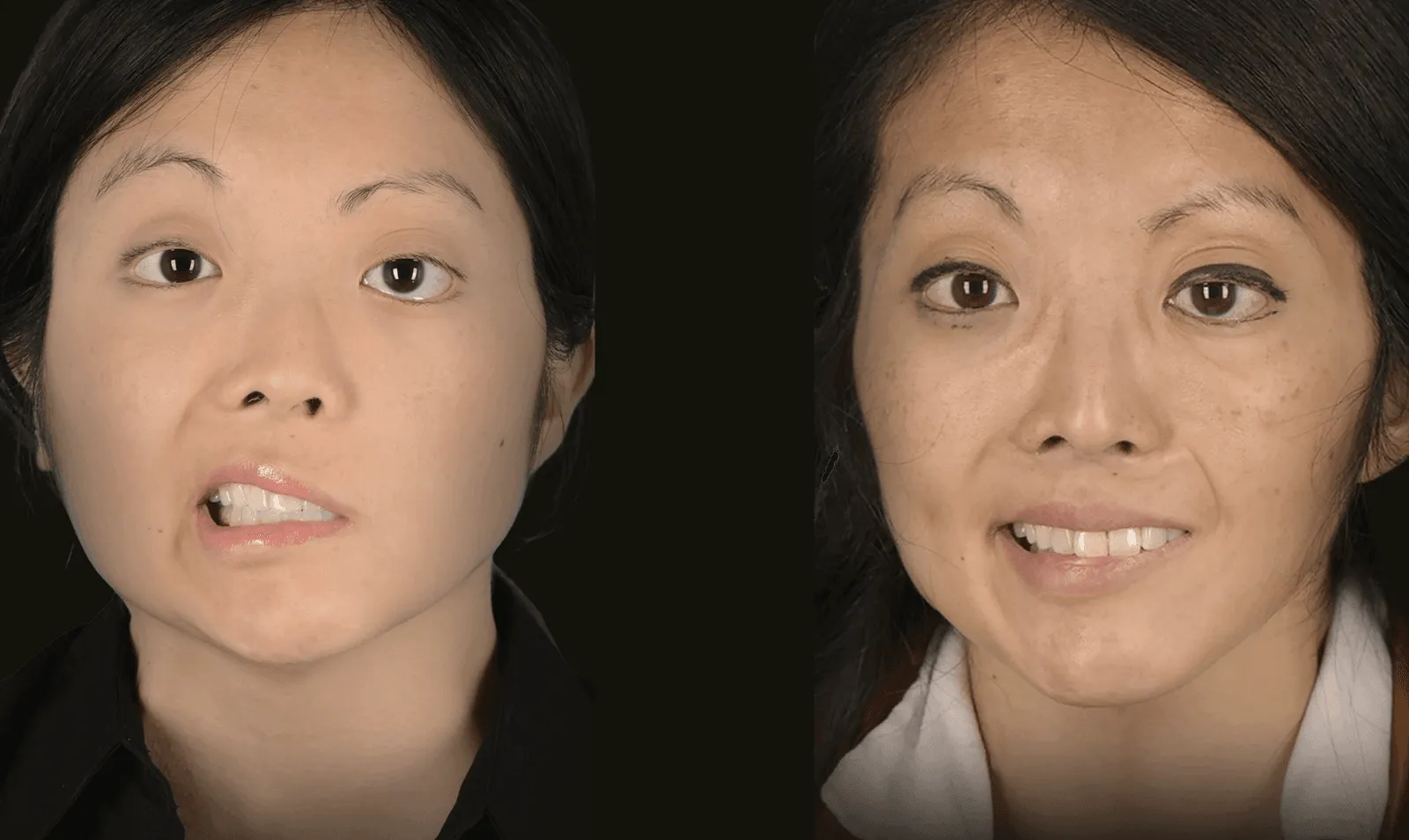
The Outcome
One year after surgery, the patient has regained excellent facial tone and the ability to smile symmetrically. The eye closes more fully, reducing the risk of eye infections. The movement is strong and becomes more natural as the patient learns to coordinate the new nerve inputs.