Multi-Stage Restoration After Brainstem Tumor
A staged approach to bringing back a smile.

At a Glance
The Challenge
Following the removal of a tumor on the brainstem, this patient was left with facial paralysis. Because the damage occurred at the brainstem level, the main facial nerve was not viable for direct repair, requiring a creative, multi-step solution to restore movement.
The Solution
Dr. Jowett adopted a multi-stage approach. Initially, nerves from the shoulder and neck were rerouted to provide a source of neural energy to the face. In a subsequent stage, a small muscle from the inner thigh (gracilis) was transplanted to the face and connected to these new nerve sources. This "free muscle transfer" acts as a new motor to power the smile.
Technical Insight
Procedure: Spinal accessory and cervical nerve transfers, followed by free gracilis muscle transfer.
Surgical Note: Brainstem pathology often precludes the use of the proximal facial nerve stump. In such cases, extra-facial motor donors are required. A staged approach allows for pre-conditioning or direct neurotization. Here, the spinal accessory nerve and cervical plexus branches were utilized to power a free gracilis muscle flap, providing robust excursion for smile reconstruction.
First Stage Surgery: Nerve Transfers
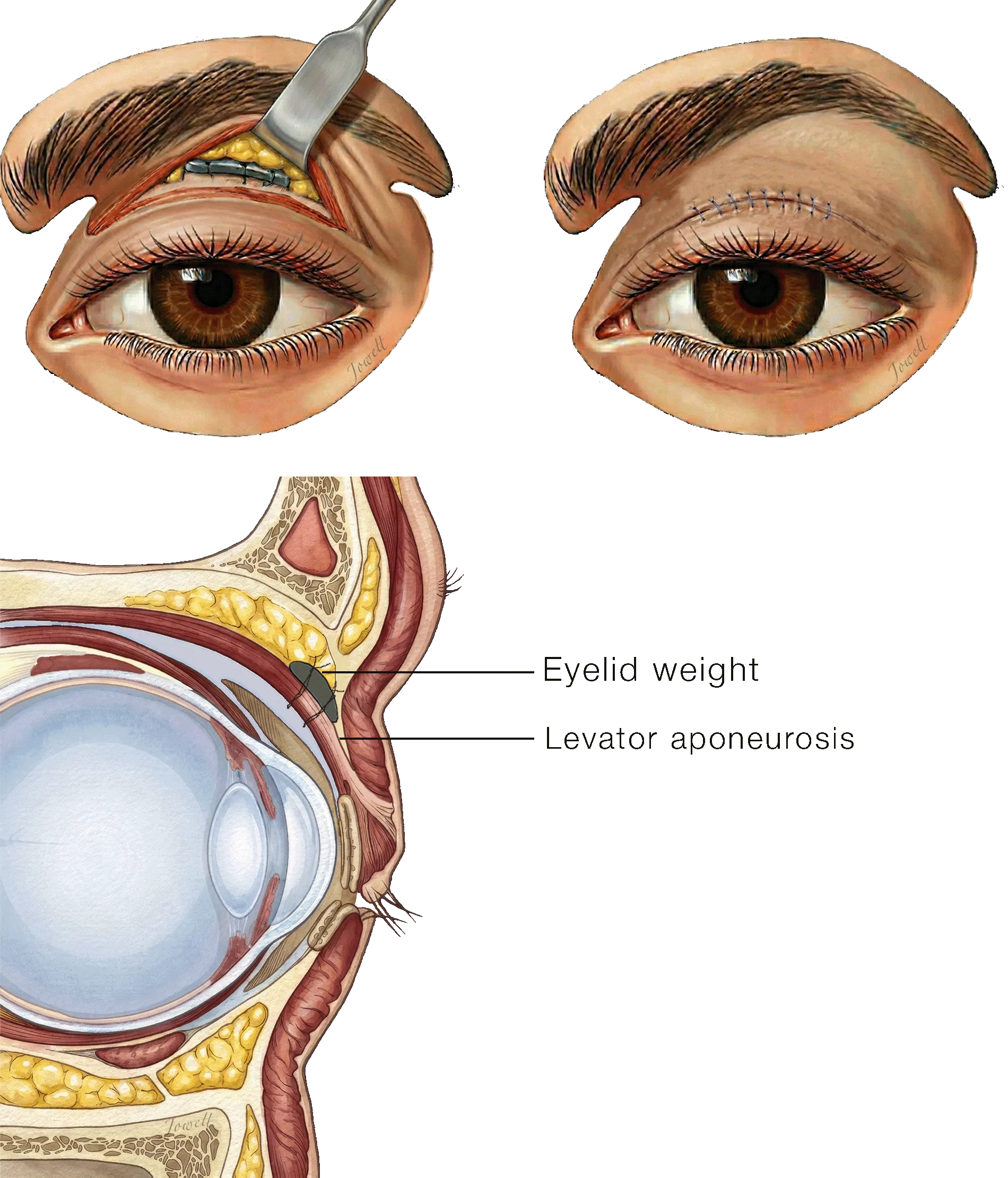
Upper Eyelid Weighting in Facial Paralysis
Through a discreet incision in the upper eyelid crease, a thin platinum weight is inserted to assist with eyelid closure. The weight is placed deep beneath the skin and fat of the upper eyelid so it remains invisible.
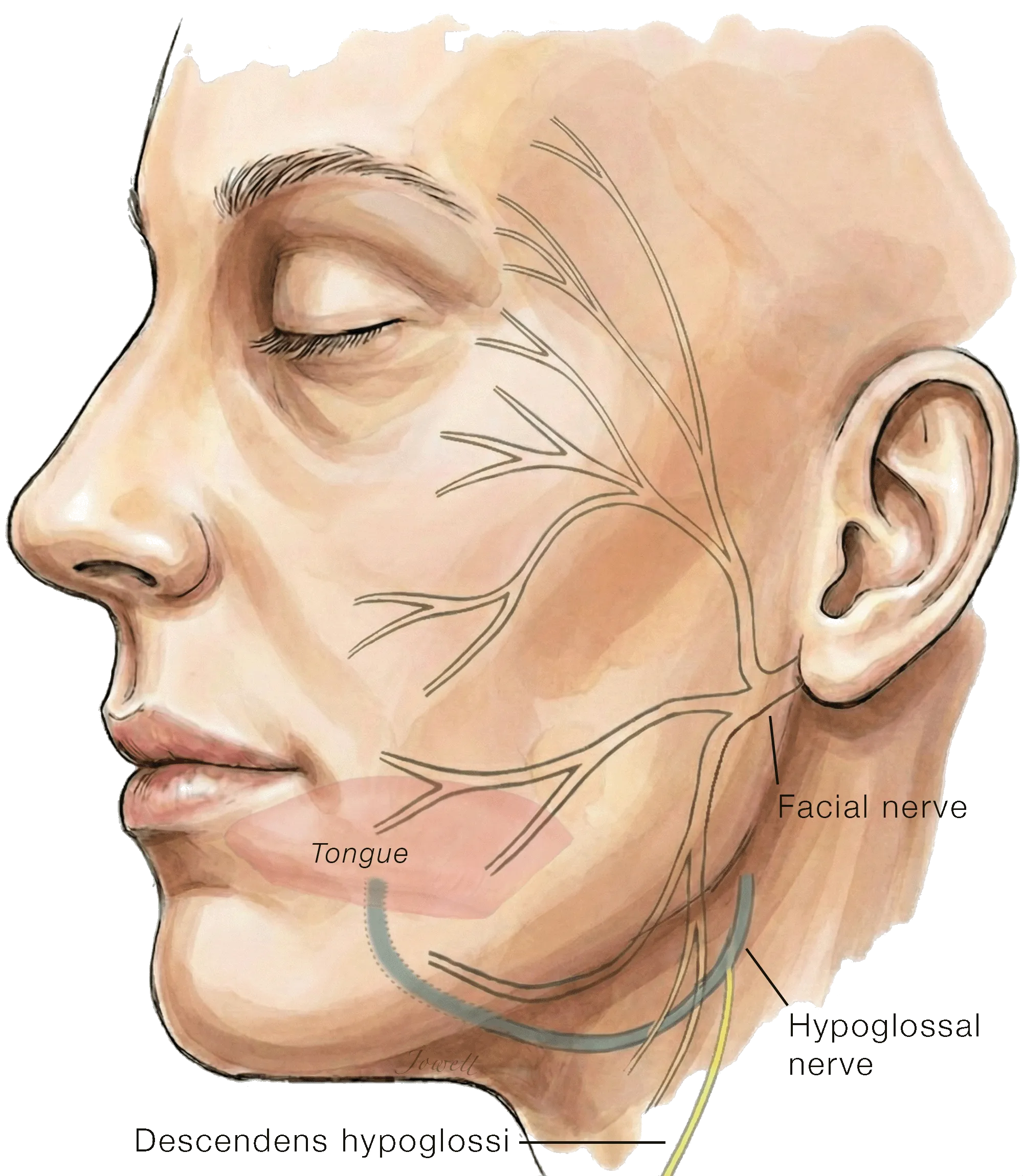
Donor Options for Nerve Transfer in Facial Reanimation
In facial paralysis resulting from injury to the facial nerve near the brainstem, the nerve no longer delivers electrical signals to the muscles of expression. However, the nerve branches within the face itself remain healthy and intact, ready to be reconnected to new power sources to restore tone and movement.
The Hypoglossal Nerve: Located just below the jaw, this nerve controls movement of the tongue. Because of its close proximity and natural redundancy, a portion of this nerve is often used as a 'donor' to restore muscle tone and movement to the face.
The Descendens Hypoglossi Nerve: This nerve controls movement of small muscles in the neck and can serve as an additional power source to restore resting tone to the paralyzed side.
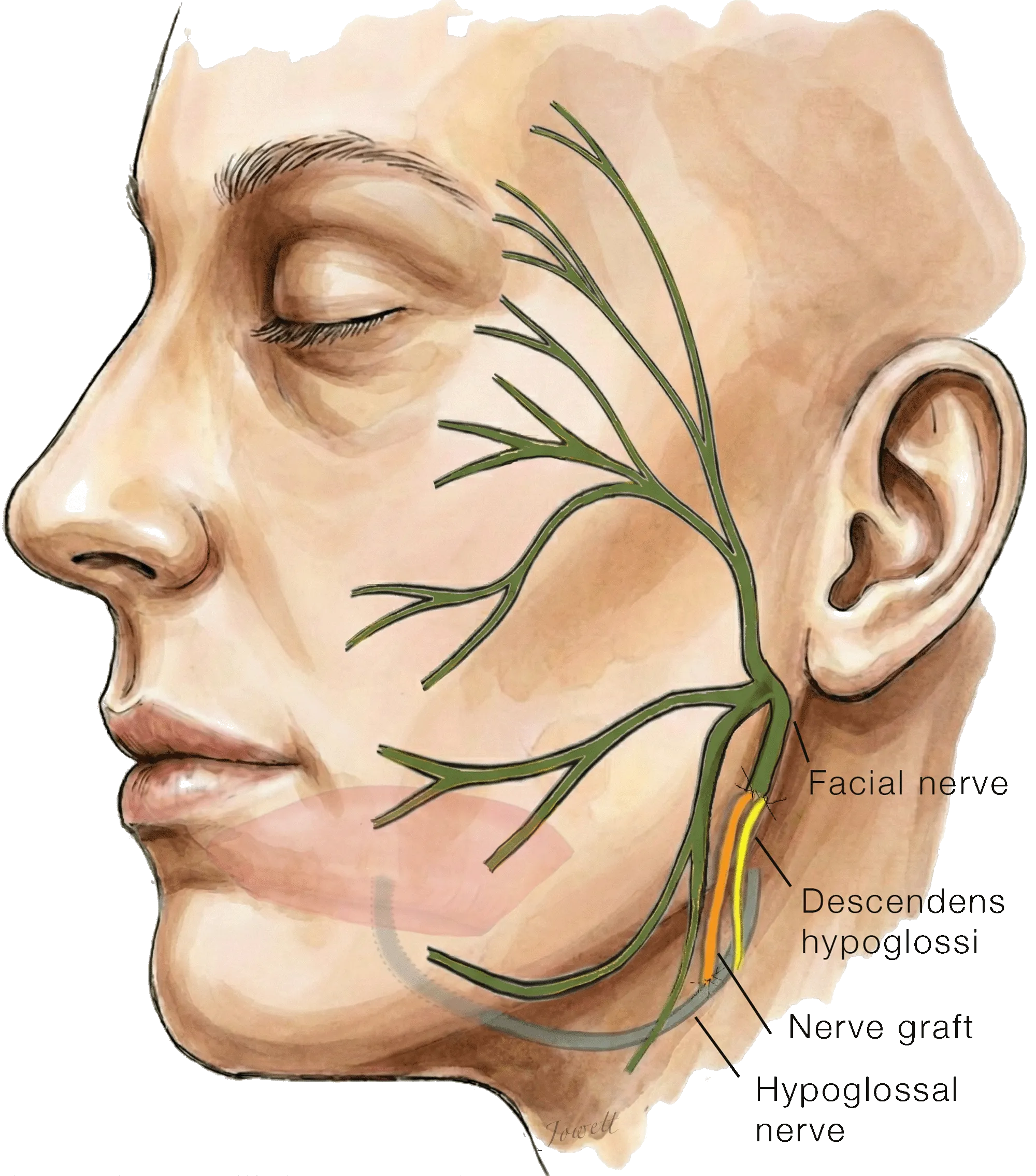
Hypoglossal and Descendens Hypoglossi Transfer to Facial Nerve
A proportion of nerve fibers within the hypoglossal nerve supplying tongue movements are rerouted using a nerve graft (orange) to the main trunk of the facial nerve. Additionally, the descendens hypoglossi nerve (yellow) is also connected to provide additional power to the muscles of facial expression. This combination helps restore resting symmetry and some movement to the paralyzed side of the face.
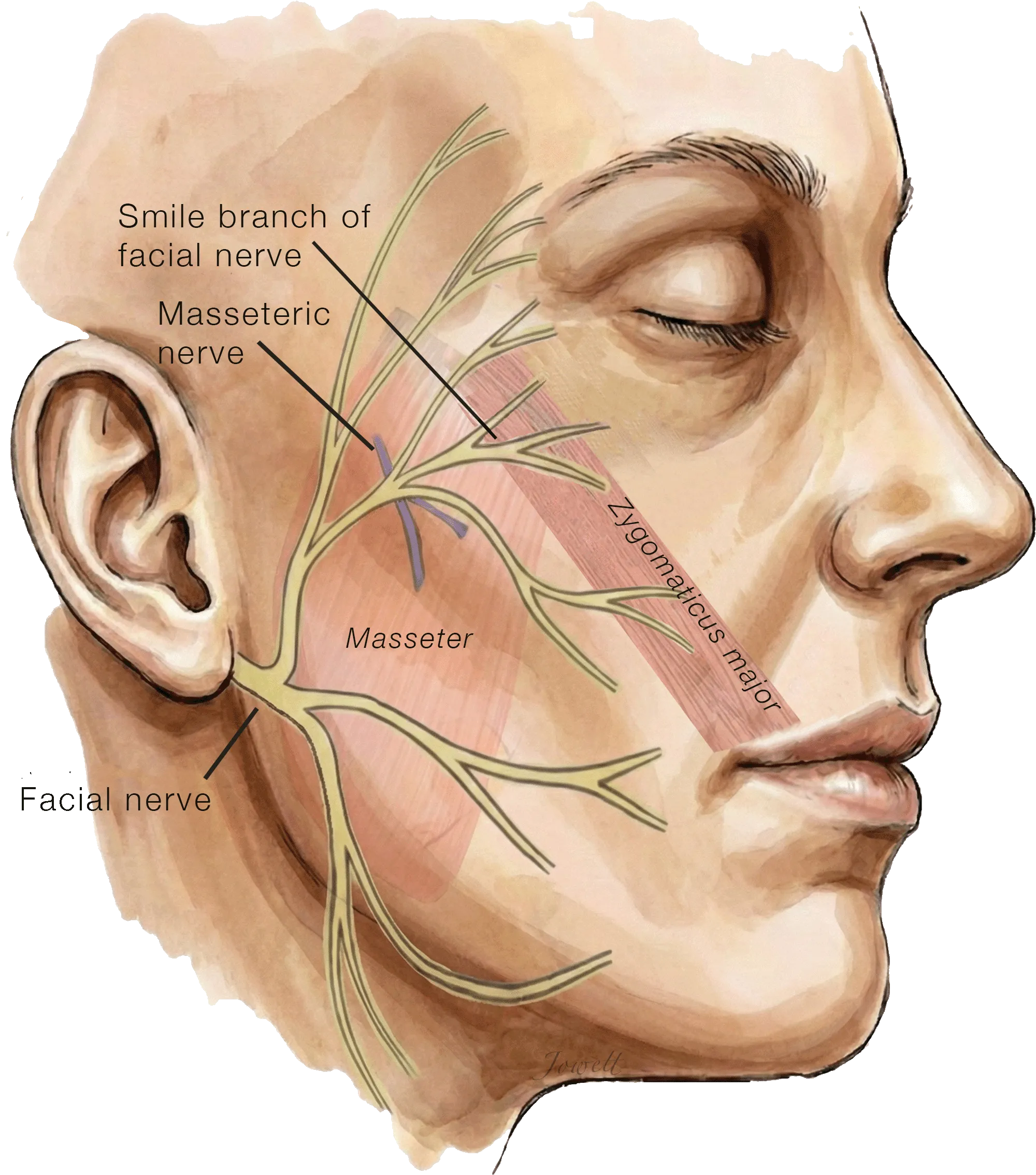
Cross-Facial Nerve Grafting Donor Nerves
This diagram illustrates the anatomy on the unaffected (healthy) side of the face. To restore a smile on the paralyzed side, we identify two distinct 'power sources' on this healthy side:
Smile activity: A redundant branch of the facial nerve supplying the primary smile muscle (zygomaticus major muscle).
Chewing activity: A branch of the nerve supplying the masseter muscle (masseteric nerve).
After surgically locating these specific distal branches, we prepare to connect them to a nerve graft bridge that will carry their signals across the face to power smile movements on the paralyzed side.
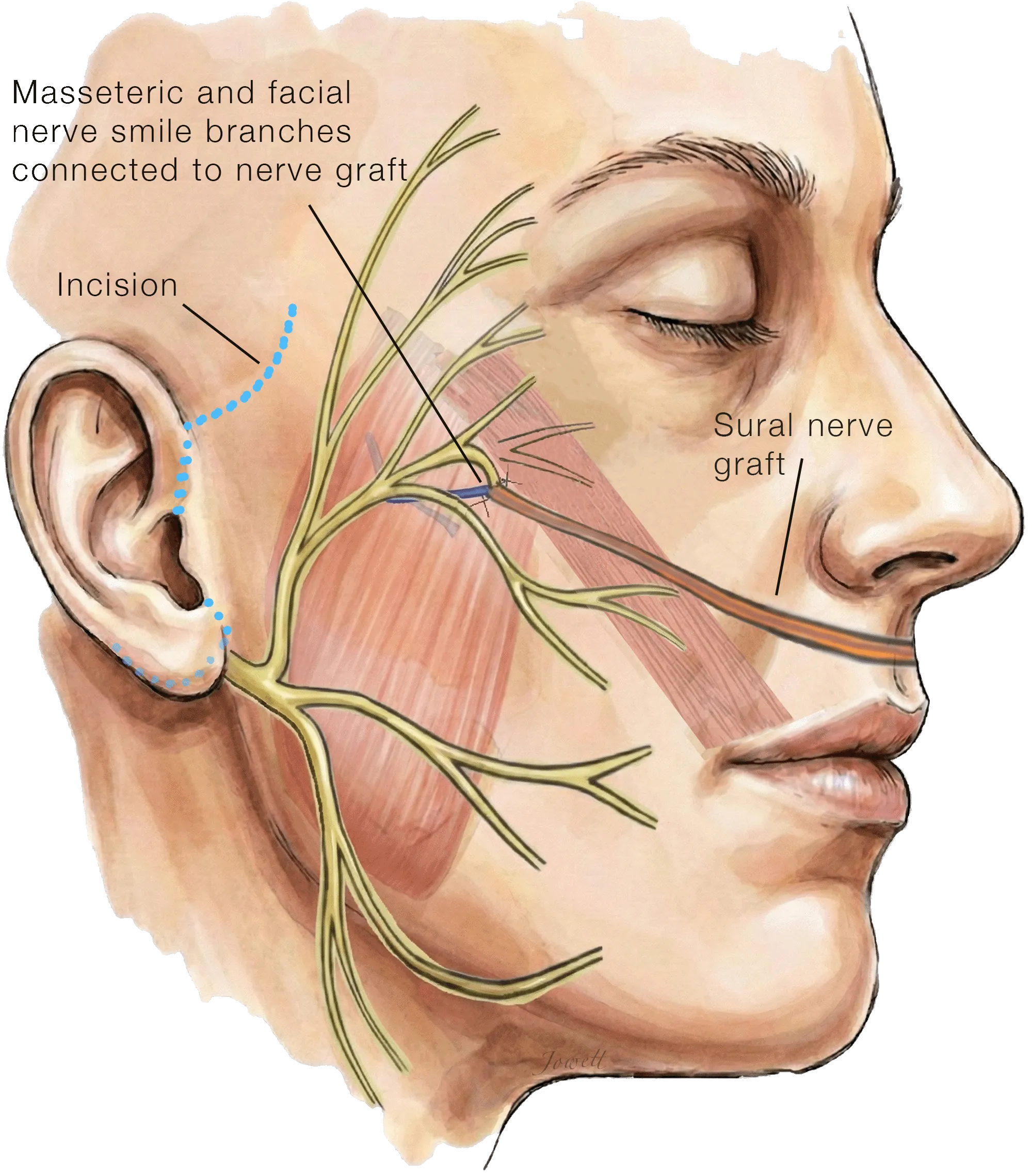
Masseteric-Supercharged Cross-Facial Nerve Graft
The long nerve graft harvested from the lower leg is tunneled under the skin across the upper lip via a facelift incision and connected to the two 'power sources': the smile branch and the chewing branch.
Over the next several months, nerve fibers from the healthy side will grow across the nerve graft, where they will later power muscle transferred from the thigh to the face with the spontaneity of a natural smile and the strength of the chewing nerve.
Second Stage Surgery: Muscle Transfer
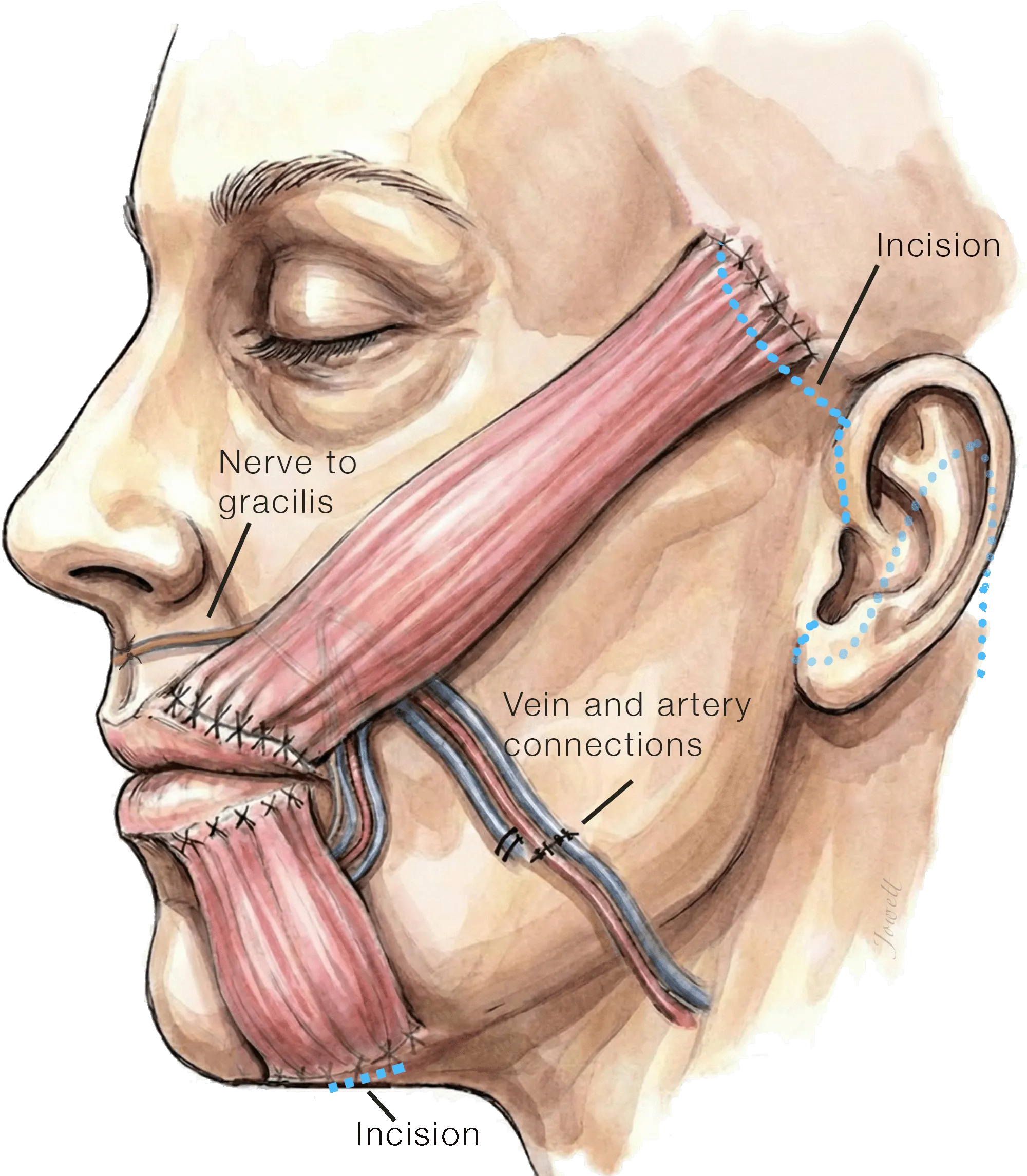
Dual-Vector Free Gracilis Muscle Transfer for Smile Reanimation Neurotized by Ipsilateral Masseteric Nerve
After a delay of several months to allow nerve fibers to grow across the nerve graft, a small strip of gracilis muscle is taken from the thigh, divided into two parts, and carefully placed into the face to rebuild the smile. This is done through a well-camouflaged facelift incision, along with small incisions inside the mouth and under the chin.
The Outcome
One year after completing the reconstruction, the patient has a functional, voluntary smile. The transplanted muscle contracts effectively, lifting the corner of the mouth and restoring a more symmetrical and expressive appearance.