Repairing the Facial Nerve After Cancer Surgery
Microsurgical reconstruction following salivary gland cancer removal.

At a Glance
The Challenge
Surgery to remove a cancer of the parotid (salivary) gland often places the facial nerve at high risk, as the nerve runs directly through the gland. In this case, the cancer surgery required the removal of a section of the facial nerve, resulting in immediate paralysis of the corresponding facial muscles.
The Solution
To restore function, Dr. Jowett performed an immediate microsurgical repair. He used a nerve graft (a segment of sensory nerve taken from elsewhere in the body) to bridge the gap created by the cancer removal. He painstakingly repaired eight separate branches of the facial nerve, reconnecting the brain's signals to the muscles of the face.
Technical Insight
Procedure: Cable nerve grafting to eight distal facial nerve branches.
Surgical Note: Immediate reconstruction of facial nerve defects yields the best functional outcomes. In this radical parotidectomy defect, a branching pattern of autologous nerve grafts (typically great auricular or sural) was used to reapproximate the proximal facial nerve stump to eight individual distal branches, restoring tone and movement to multiple facial zones.
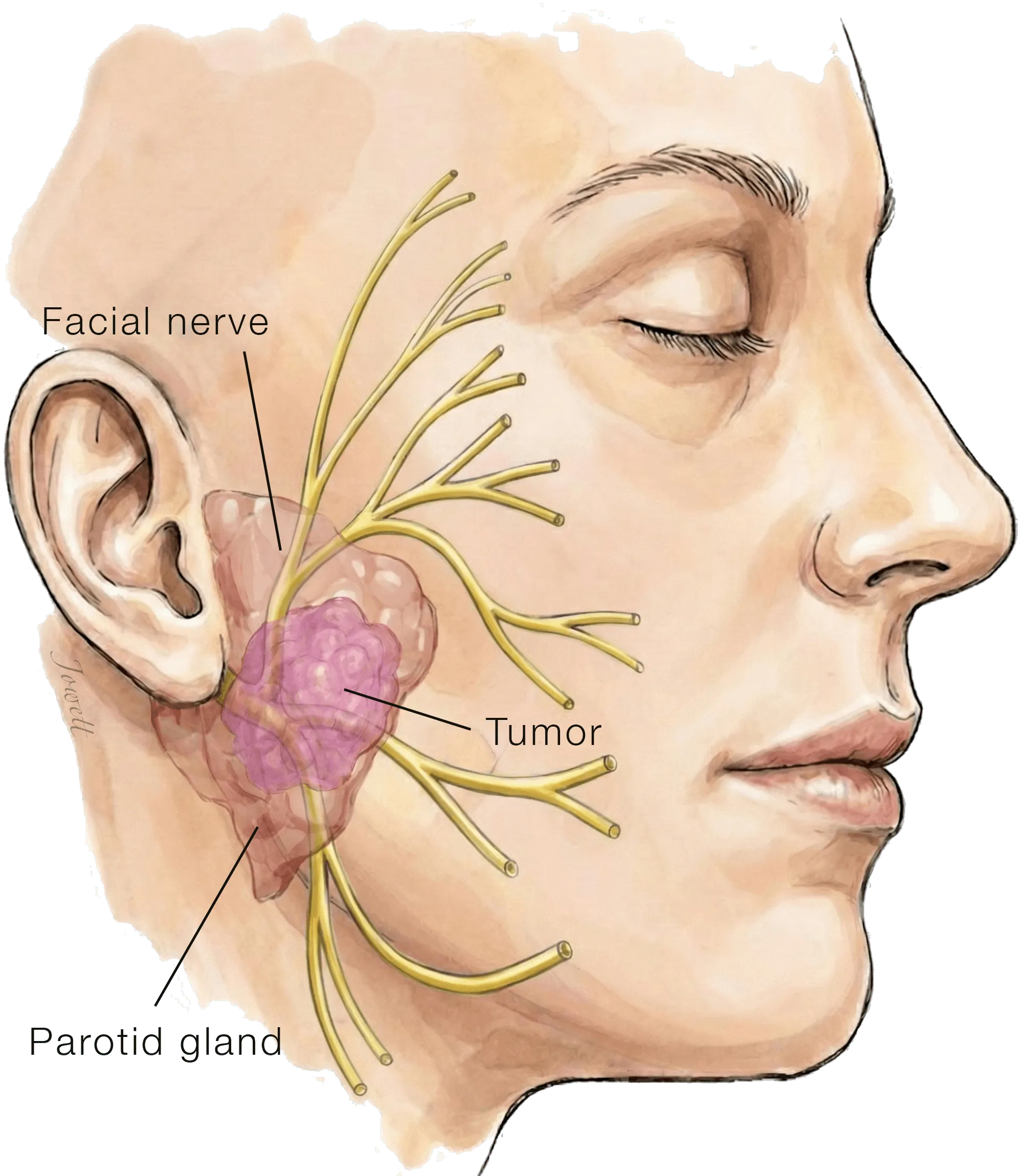
Cancer of the Parotid Gland
Cancerous tumors of the parotid gland, a large salivary gland in the cheek, often involve the facial nerve, which runs through the center of the gland.
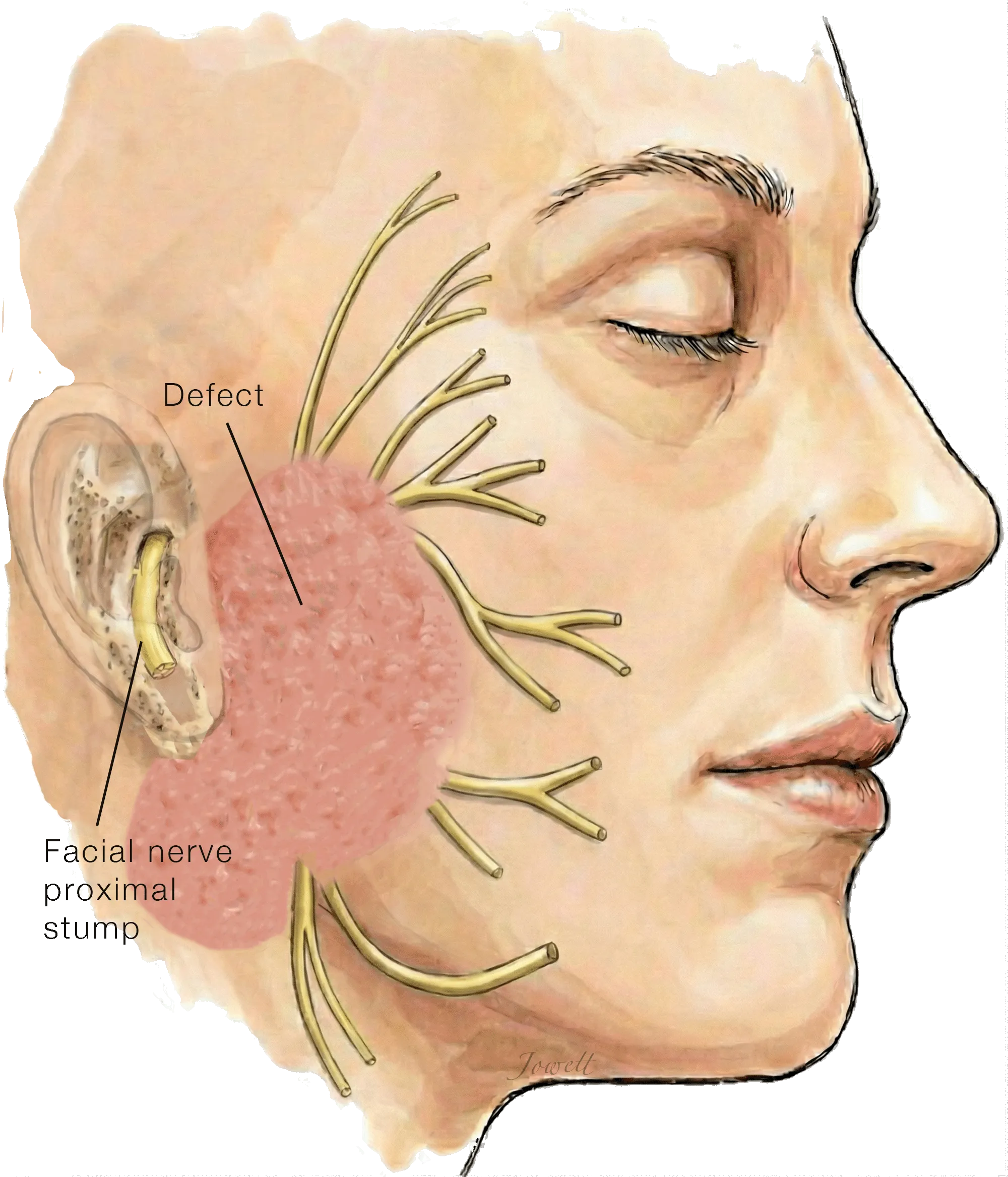
Radical Parotidectomy
Treatment of parotid cancer often requires "radical parotidectomy", where the entire parotid gland is removed together with segments of facial nerve coursing within it, resulting in dense facial paralysis.
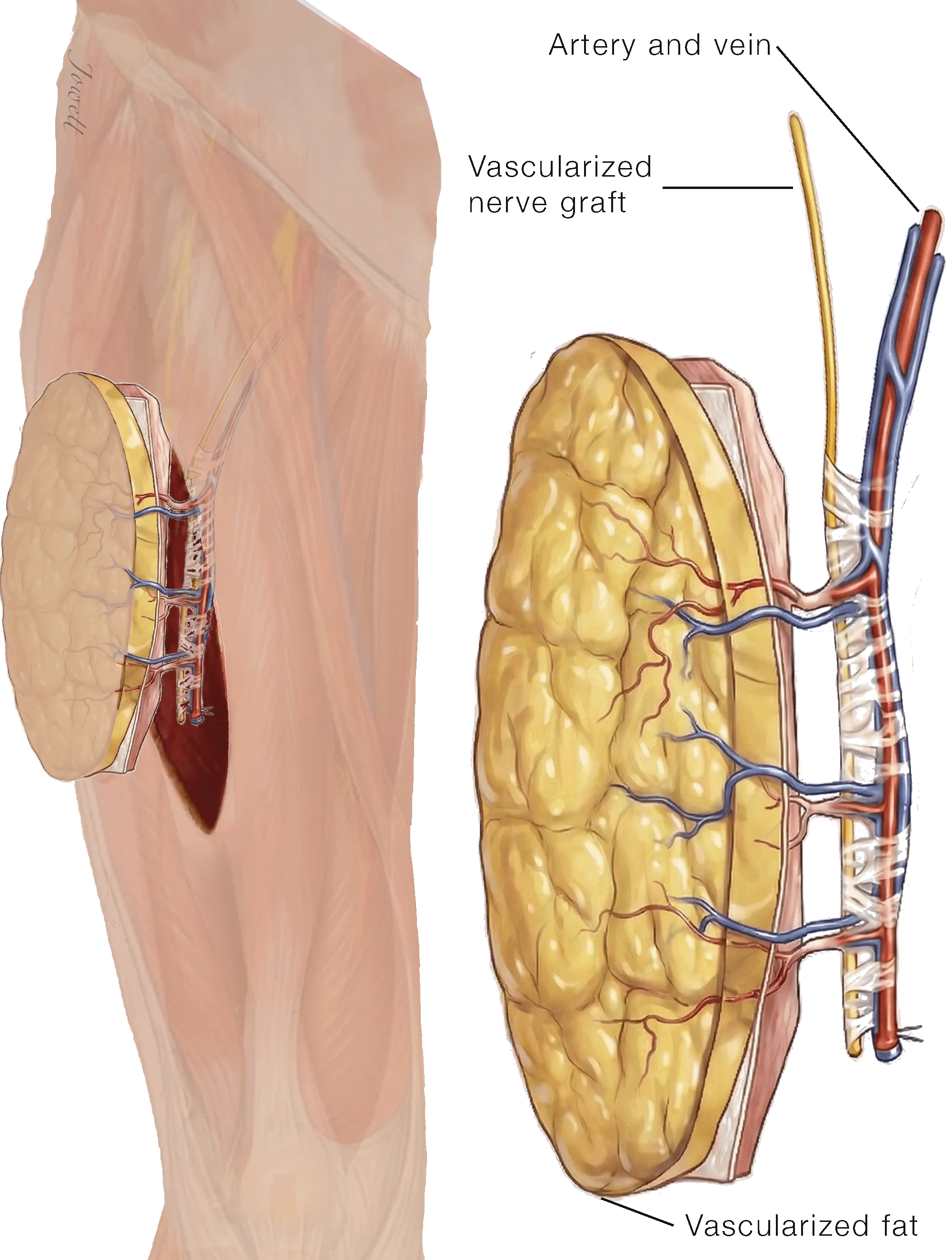
Anterolateral Thigh Flap
Through an incision on the outer thigh, a segment of soft tissue containing fat and nerve is removed. The fat is then transferred to the face and kept alive by reconnecting its blood vessels to blood vessels in the face, while the nerve graft is used to repair the facial nerve.
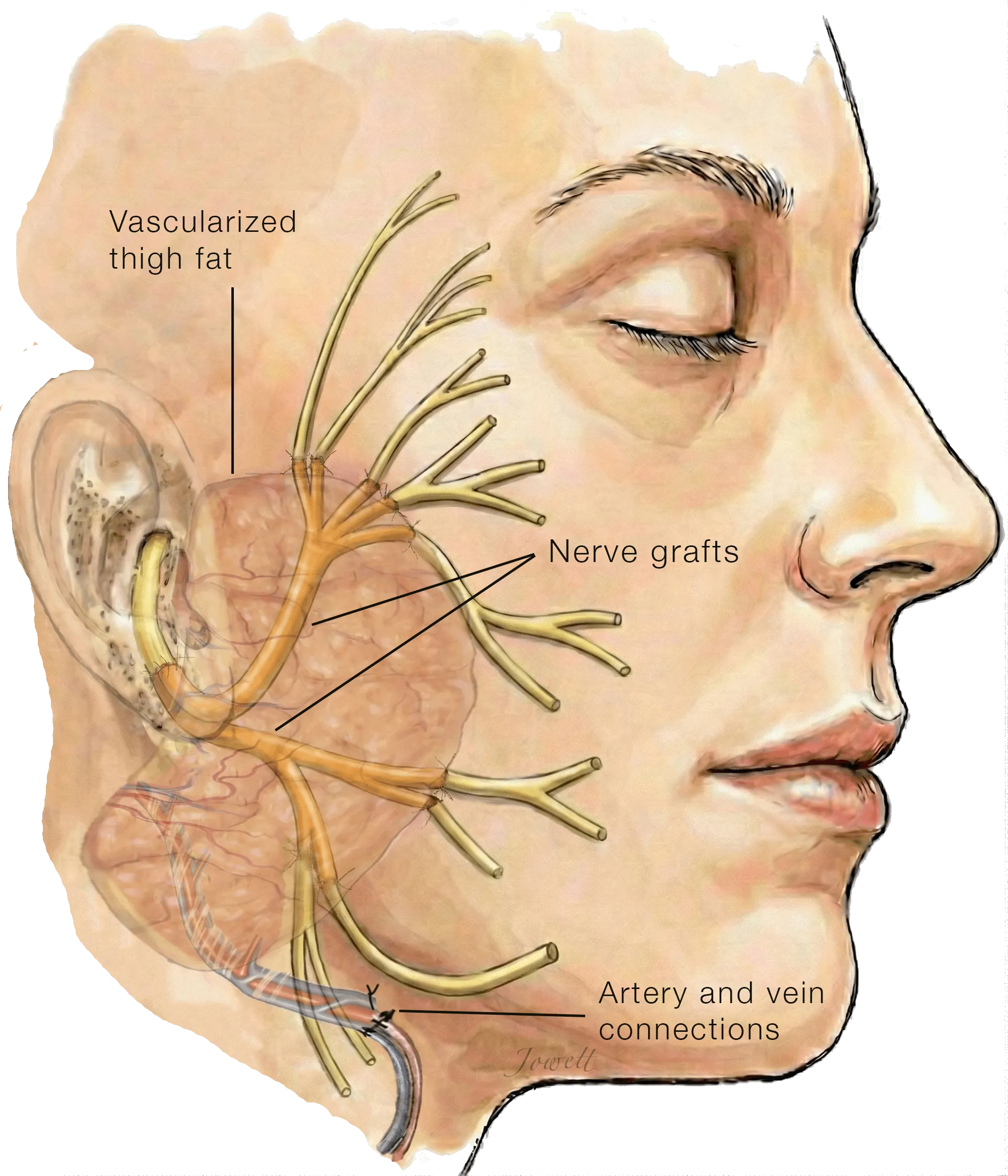
Interposition Graft Repair of Facial Nerve and Recontouring
Nerve and fatty tissue from the thigh are transferred to the face. The nerve graft is divided into small strands and used to bridge the gap between the main facial nerve and its smaller branches. The fatty tissue is then placed into the void under the skin flap to restore a natural cheek contour, and is kept alive by reconnecting its blood vessels to those in the face.
The Outcome
One year after surgery, the patient has regained excellent facial movement. The nerve grafts have successfully integrated, allowing the patient to smile, close their eye, and express themselves naturally, minimizing the visible impact of the cancer surgery.