Comprehensive Reconstruction After Blood Cancer
A multi-technique approach to restore facial function and smile.

At a Glance
The Challenge
This patient experienced facial paralysis as a result of a blood cancer and its treatment. The loss of facial nerve function left them unable to smile or move the affected side of the face, creating functional difficulties and significant emotional distress during an already challenging recovery.
The Solution
Dr. Jowett employed a pioneering combination of techniques. First, healthy nerves that normally control shoulder movement and chewing were rerouted to re-energize the facial muscles. Additionally, a small strip of muscle from the thigh (gracilis) was transplanted to the face to specifically rebuild the smile mechanism. This "multi-vector" approach ensures both strong movement and natural resting tone.
Technical Insight
Procedure: Spinal accessory nerve transfer, masseteric nerve transfer, and free gracilis muscle transfer.
Surgical Note: This case illustrates a comprehensive, multi-modal approach for severe or long-standing paralysis. Nerve transfers (spinal accessory, masseteric) provide axonal input to native musculature where viable. The free gracilis flap adds new contractile muscle tissue to restore dynamic excursion of the oral commissure (smile) when native muscles have atrophied or require augmentation.
First Stage Surgery: Multiple Nerve Transfers
Accessory to Facial Nerve Transfer for Facial Reanimation
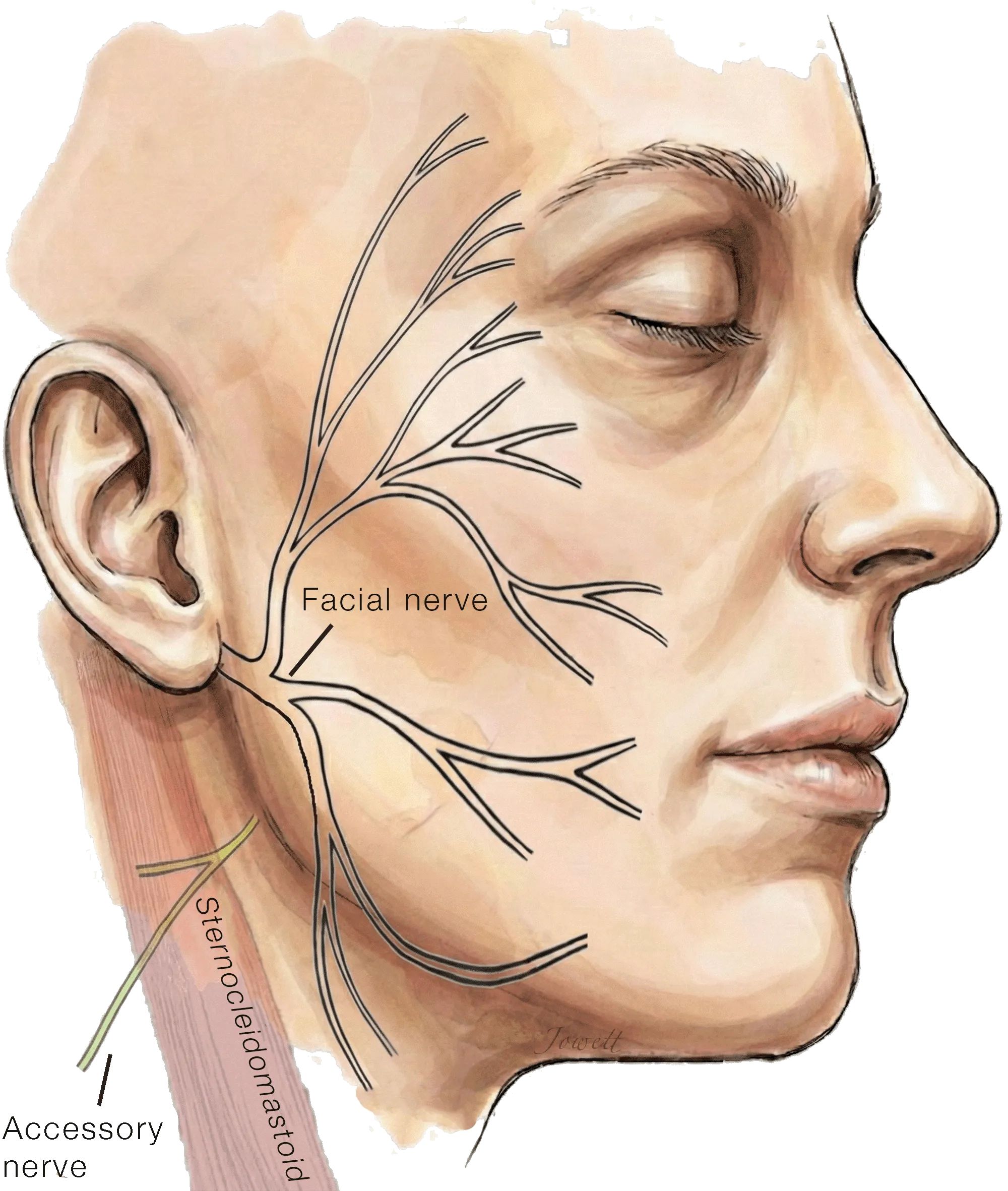
In facial paralysis resulting from injury to the facial nerve near the brainstem, the nerve no longer delivers electrical signals to the muscles of expression. However, the nerve branches within the face itself remain otherwise intact, ready to be reconnected to new power sources to restore tone and movement.
Common sources include the hypoglossal and masseteric nerves; however, in patients who already have difficulty swallowing and/or chewing, the accessory nerve can be a preferred choice for use as a donor nerve. Located in the upper neck, the accessory nerve supplies large muscles of the neck (sternocleidomastoid) and shoulder region (trapezius). Because of its proximity and redundancy, a branch of this nerve may be used as a 'donor' to restore muscle tone and movement without compromising speech, swallowing, or shoulder function.
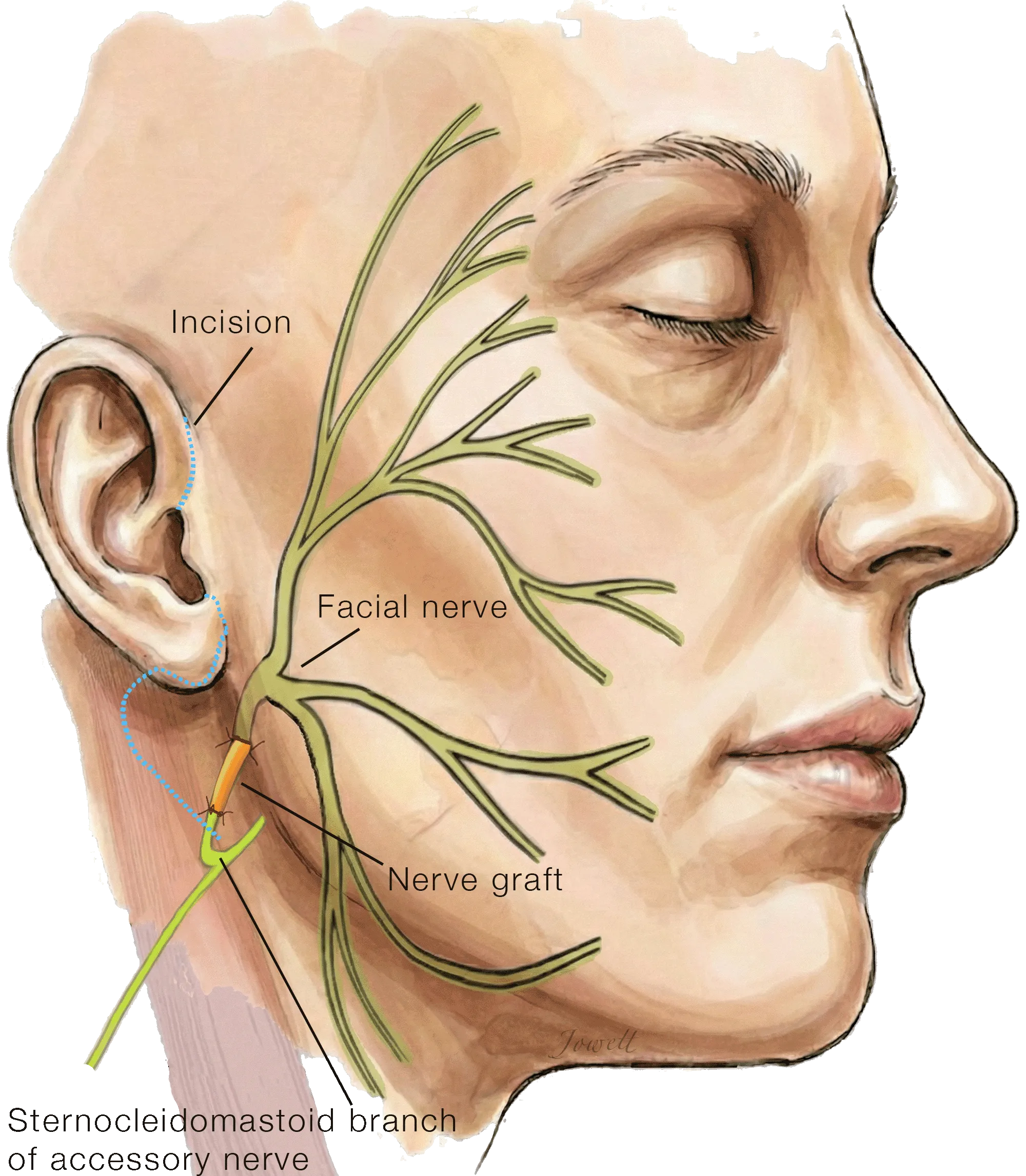
Accessory to Facial Nerve Transfer for Facial Reanimation
Through a small incision, a branch of the accessory nerve carrying fibers that supply the sternocleidomastoid muscle in the neck are rerouted, using a small nerve graft, to the muscles of facial expression to improve facial tone and symmetry without impacting shoulder function.
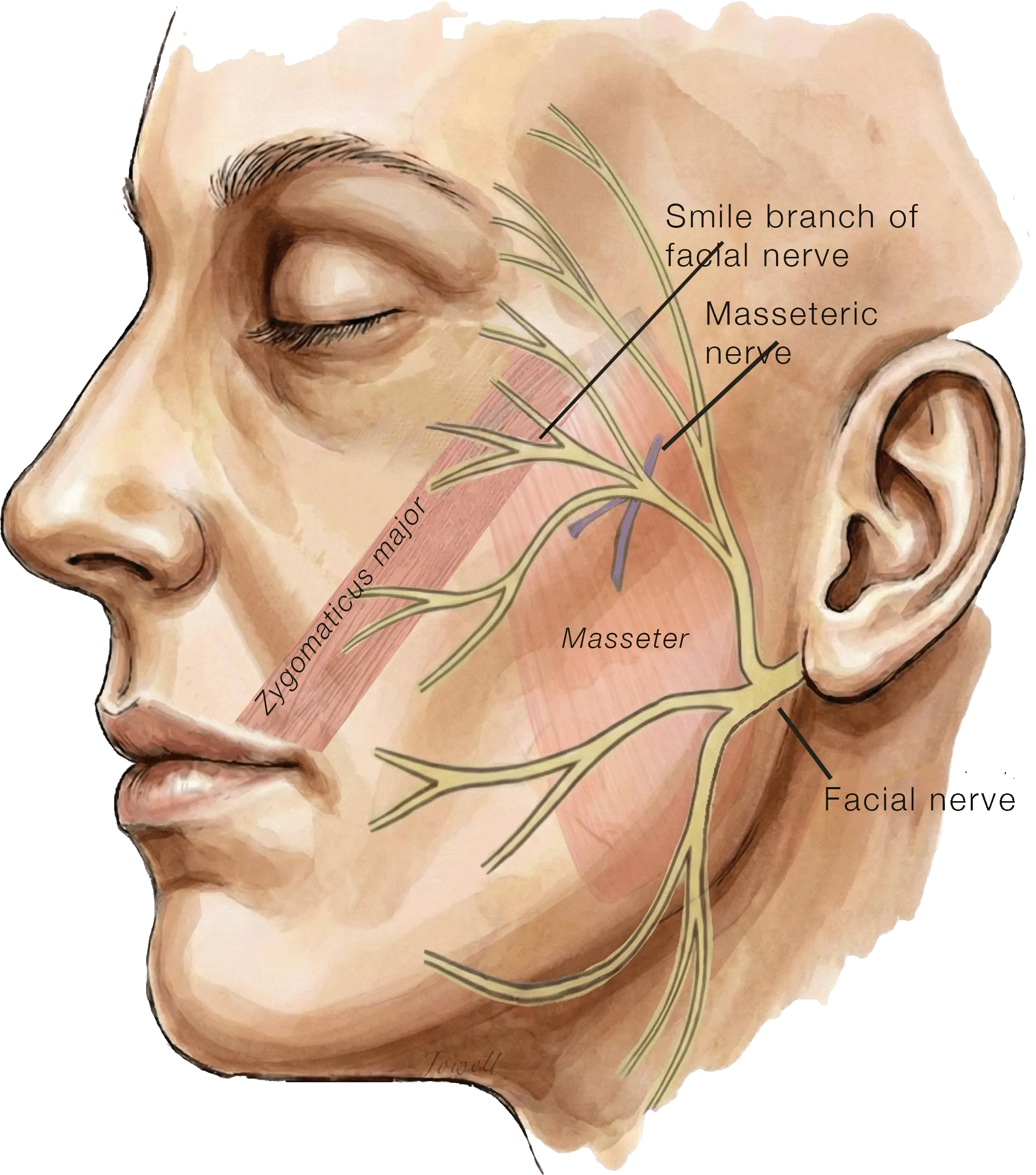
Cross-Facial Nerve Grafting "Donor" Nerves
This diagram illustrates the anatomy on the unaffected (healthy) side of the face. To restore a smile on the paralyzed side, we identify two distinct 'power sources' on this healthy side:
Smile nerve: A redundant branch of the facial nerve connected to the smile muscle (Zygomaticus major).
Chewing nerve: A branch of the nerve used for chewing (masseter nerve).
After surgically locating these specific distal branches, we prepare to connect them to a nerve graft bridge that will carry their signals across the face to power smile movements on the paralyzed side.
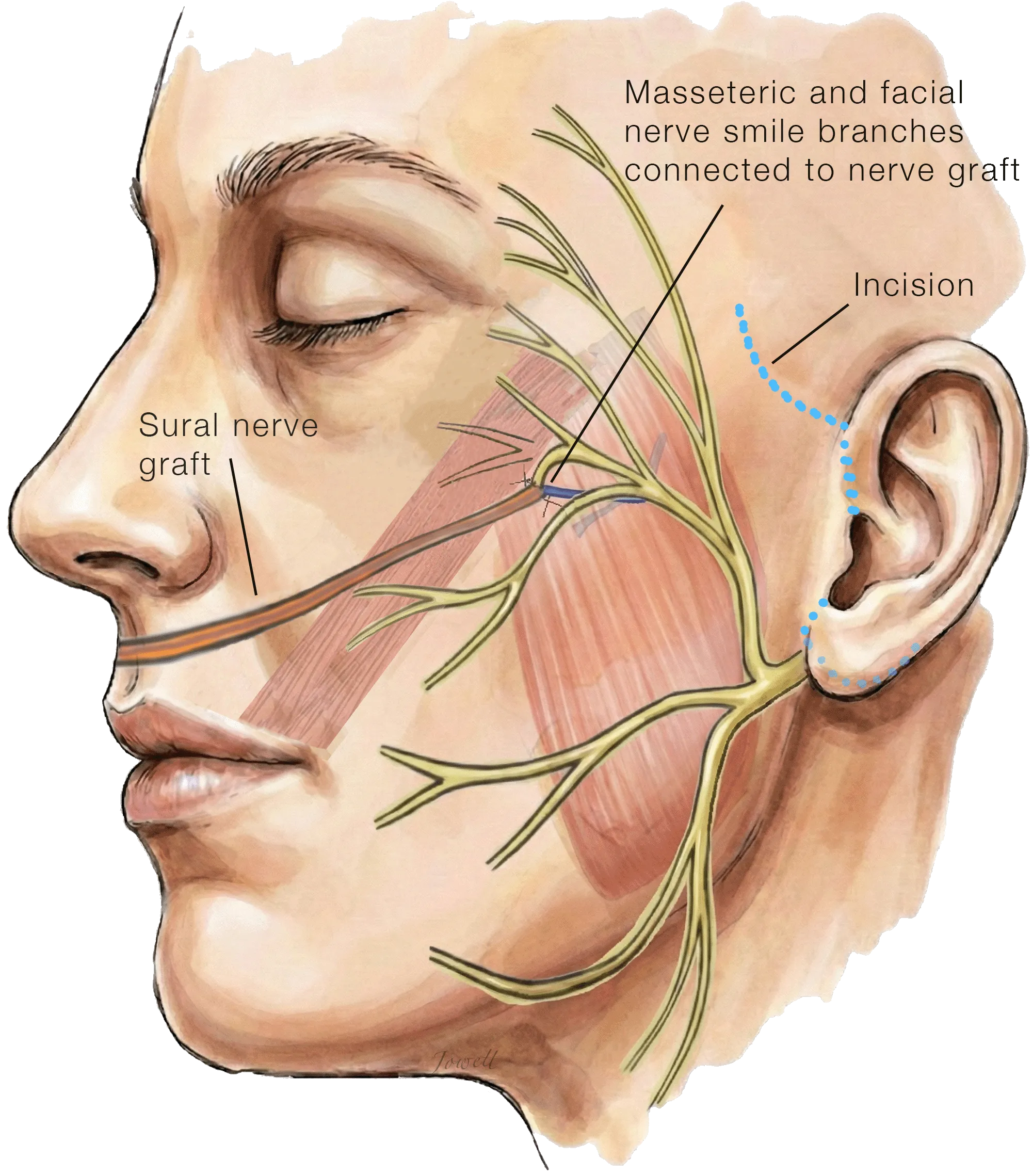
Masseteric-Supercharged Cross-Facial Nerve Graft
The long nerve graft harvested from the lower leg is tunneled under the skin across the upper lip via a facelift incision and connected to the two 'power sources': the smile branch and the chewing branch.
Over the next several months, nerve fibers from the healthy side will grow across the nerve graft, where they will later power muscle transferred from the thigh to the face with the spontaneity of a natural smile and the strength of the chewing nerve.
Second Stage Surgery: Functional Muscle Transfer for Smile Reanimation
Dual-Vector Free Gracilis Muscle Transfer for Smile Reanimation Neurotized by Cross-Facial Nerve Graft
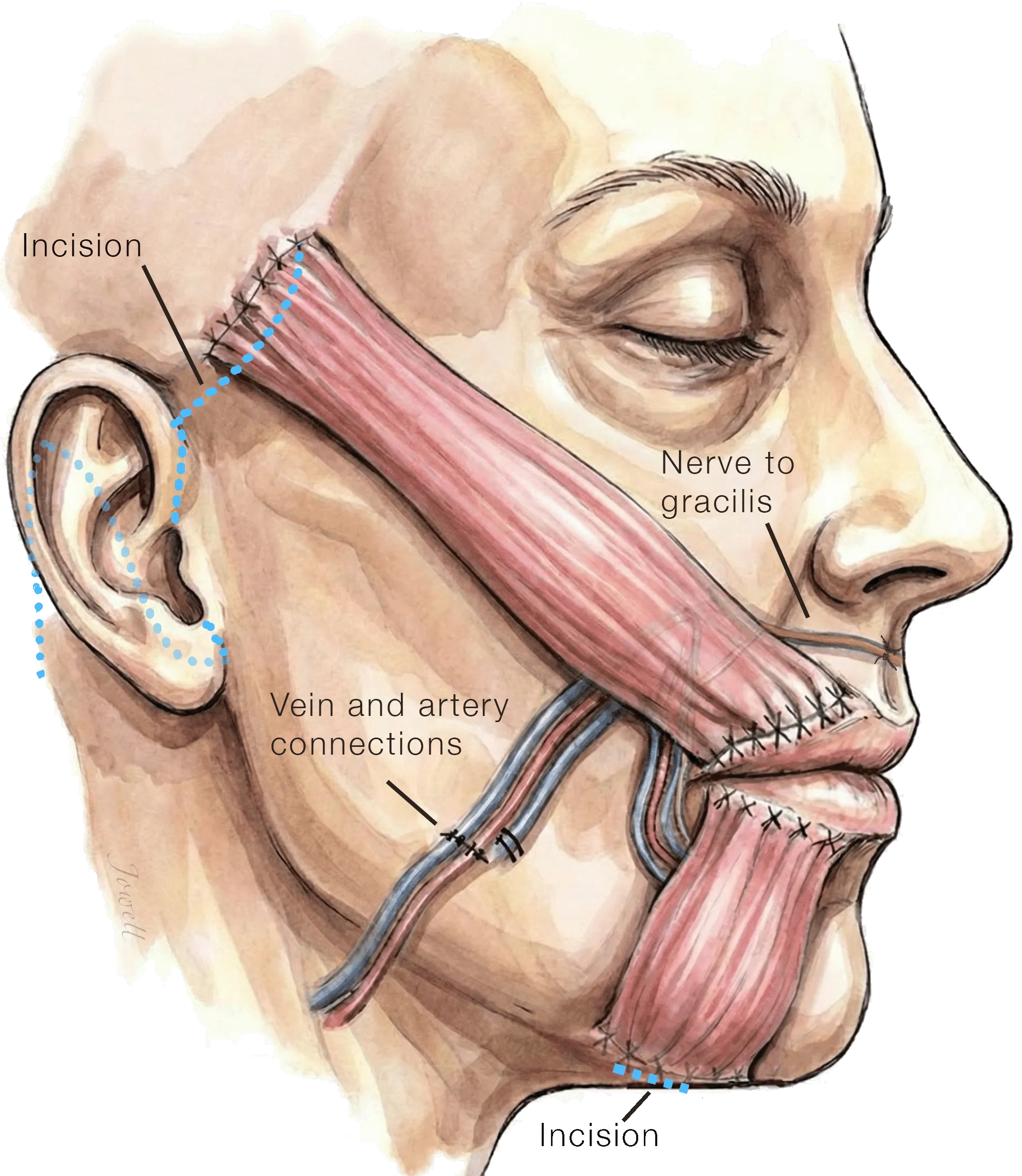
After a delay of several months to allow nerve fibers to grow across the nerve graft, a small strip of gracilis muscle is taken from the thigh, divided into two parts, and carefully placed into the face to rebuild the smile. This is done through a well-camouflaged facelift incision, along with small incisions inside the mouth and under the chin.
The muscle’s artery and vein are then connected to blood vessels in the face, and its nerve is connected to the cross-facial nerve graft that was placed during the first stage of surgery.
The Outcome
One year after the final stage of reconstruction, the patient has achieved a remarkable restoration of facial symmetry and expression. The smile is broad and natural, and the overall facial tone is balanced, helping the patient return to normal life with renewed confidence.